Introduction
Gestational Diabetes Mellitus (GDM) is a form of glucose intolerance that develops during pregnancy, usually in the second or third trimester. It occurs when the body cannot adequately compensate for the increased insulin resistance of pregnancy. With early diagnosis, structured nutritional therapy, and close medical supervision, most women with GDM can achieve healthy pregnancy outcomes.
Physiology of Gestational Diabetes
4
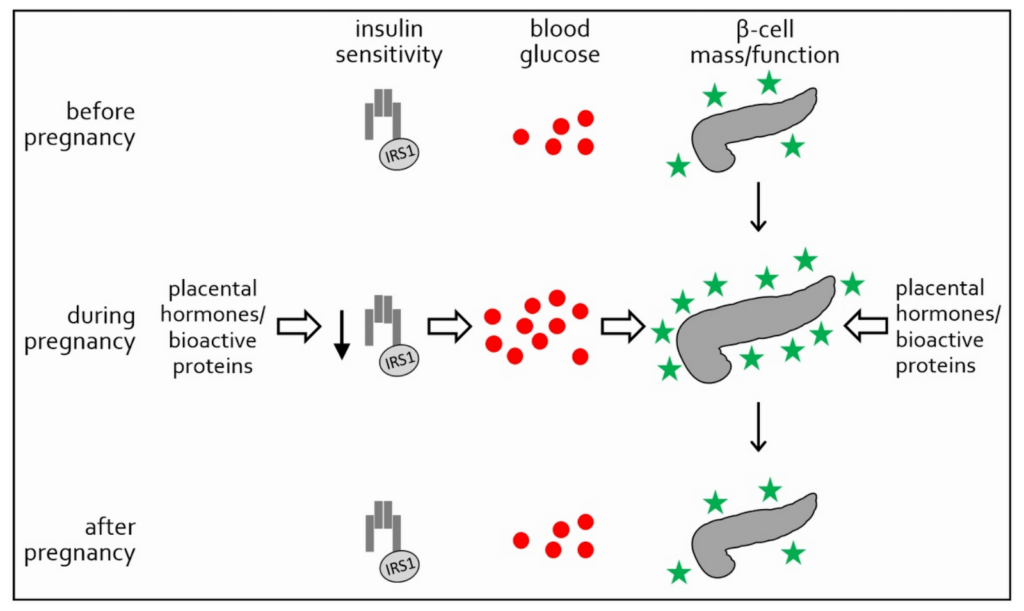
1. Normal Metabolic Changes in Pregnancy
Pregnancy is a diabetogenic state by design. To ensure a continuous glucose supply to the fetus:
- Maternal insulin sensitivity decreases
- Hepatic glucose production increases
- Fat metabolism rises to spare glucose for the fetus
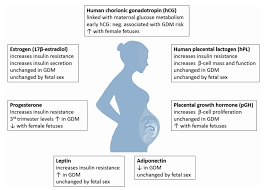
These changes are mainly driven by placental hormones such as:
- Human placental lactogen (hPL)
- Progesterone
- Estrogen
- Cortisol
- Placental growth hormone
2. Development of GDM
In healthy pregnancies, pancreatic β-cells increase insulin secretion to compensate for insulin resistance.
GDM develops when:
- β-cell compensation is insufficient
- Pre-existing insulin resistance is unmasked
Key physiological features:
- Reduced glucose uptake by skeletal muscle and adipose tissue
- Increased postprandial hyperglycemia
- Elevated fasting glucose due to hepatic insulin resistance
- Chronic low-grade inflammation and oxidative stress
3. Risk Factors
- Overweight or obesity
- Polycystic ovary syndrome (PCOS)
- Family history of type 2 diabetes
- Advanced maternal age
- Previous GDM or macrosomic baby
- Vitamin D deficiency and dyslipidemia
Nutritional Intervention in GDM
(Always under medical and dietetic supervision)
Nutrition therapy is the cornerstone of GDM management and aims to maintain euglycemia while supporting fetal growth.
1. Goals of Medical Nutrition Therapy (MNT)
- Achieve target blood glucose levels
- Prevent ketosis
- Ensure adequate maternal and fetal nutrition
- Avoid excessive gestational weight gain
2. Carbohydrate Management
Carbohydrates should be controlled, not eliminated.
Key principles:
- 40–50% of total calories from carbohydrates (individualized)
- Preference for low glycemic index (GI) carbohydrates
- Even distribution across meals
Recommended sources:
- Whole grains (millets, oats, brown rice in measured portions)
- Legumes and pulses
- Non-starchy vegetables
- Whole fruits (not juices)
Foods to limit or avoid:
- Refined sugars
- Fruit juices
- White bread, bakery products
- Sugary beverages
3. Protein Adequacy
Protein supports fetal growth and stabilizes postprandial glucose.
Recommended sources:
- Pulses, legumes
- Eggs, fish, lean meat (as per dietary preference)
- Dairy (curd, paneer in controlled amounts)
- Nuts and seeds
4. Healthy Fats
Fats should support insulin sensitivity and fetal brain development.
Include:
- MUFAs (mustard oil, olive oil, groundnut oil)
- Omega-3 fatty acids (flaxseed, walnuts, fatty fish)
Limit:
- Trans fats
- Deep-fried foods
5. Meal Pattern
- 3 small-to-moderate meals
- 2–3 planned snacks
- Bedtime snack to prevent nocturnal hypoglycemia and ketosis
6. Micronutrient Focus
- Iron and folate (as prescribed)
- Calcium and vitamin D
- Magnesium and zinc (support glucose metabolism)
7. Role of Physical Activity
With obstetric approval:
- 20–30 minutes of walking after meals
- Prenatal yoga or stretching
Note: A strict medical supervision is advised.
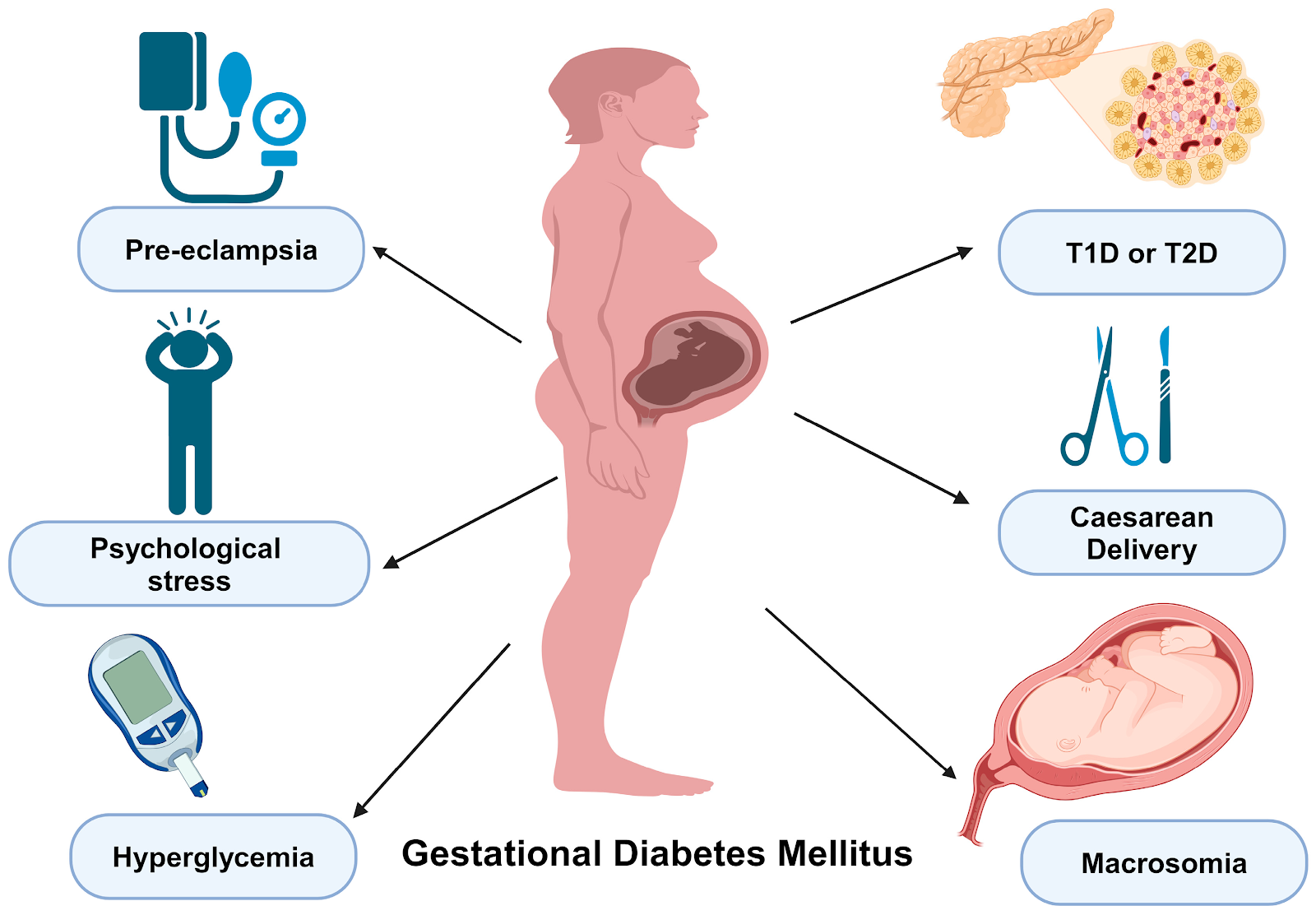
Consequences of Poorly Controlled GDM
Maternal Consequences
Short-term
- Preeclampsia
- Polyhydramnios
- Increased cesarean section risk
Long-term
- 7–10 fold higher risk of developing type 2 diabetes
- Metabolic syndrome
- Cardiovascular disease
Fetal and Neonatal Consequences
In utero
- Excess glucose transfer → fetal hyperinsulinemia
- Accelerated fat deposition
At birth
- Macrosomia
- Shoulder dystocia
- Birth trauma
- Neonatal hypoglycemia
- Respiratory distress syndrome
Long-term
- Childhood obesity
- Insulin resistance
- Type 2 diabetes in adolescence or adulthood
Importance of Medical Supervision
GDM management requires a multidisciplinary approach involving:
- Obstetrician
- Endocrinologist/physician
- Registered dietitian
- Diabetes educator
Regular monitoring includes:
- Fasting and postprandial blood glucose
- HbA1c (as advised)
- Fetal growth assessment
- Postpartum glucose testing (6–12 weeks after delivery)
Conclusion
Gestational diabetes is not merely a transient pregnancy condition—it reflects underlying metabolic vulnerability. However, with early screening, individualized nutrition therapy, lifestyle modification, and strict medical supervision, GDM can be effectively managed, ensuring optimal outcomes for both mother and baby. Moreover, postpartum follow-up and long-term lifestyle changes are crucial to breaking the intergenerational cycle of diabetes.
